

You’ve hired a talented physician. The paperwork is signed, the office is ready, and your team is eager to start seeing patients. But there is one thing standing between your new provider and a single paid claim: credentialing.
For most practices, credentialing for medical providers is simultaneously one of the most important and most frustrating administrative processes they face. Get it right, and your providers start generating revenue quickly. Get it wrong — or skip any step — and you could be looking at months of delayed billing, claim denials, and thousands of dollars in lost revenue.
This guide breaks down everything you need to know about the provider credentialing process: what it is, why it exists, how it works from start to finish, and how to avoid the pitfalls that slow most practices down.
What Is Credentialing for Medical Providers?
In simpler terms, credentialing is the healthcare industry’s official background check for clinicians. It confirms that a provider is who they say they are and that they have the qualifications, training, and clean professional history required to care for patients safely.
Credentialing applies to a wide range of healthcare professionals, including physicians (MDs and DOs), nurse practitioners and physician assistants, mental health therapists and psychologists, chiropractors, dentists, and physical and occupational therapists.
It is not optional. The Centers for Medicare and Medicaid Services (CMS) requires credentialing before a provider can be reimbursed for services rendered to Medicare or Medicaid patients. The Joint Commission on Accreditation of Healthcare Organizations (Joint Commission) mandates it for hospital-based providers. And nearly every private insurer requires it before enrolling a provider in their network.
Without completed credentialing, your practice simply cannot get paid — regardless of how many patients a provider sees.
Why Credentialing Matters for Your Practice
The stakes around credentialing are higher than most practice administrators realize until something goes wrong. Here is what is actually at risk when credentialing is delayed, incomplete, or mismanaged.
$5K–$20K
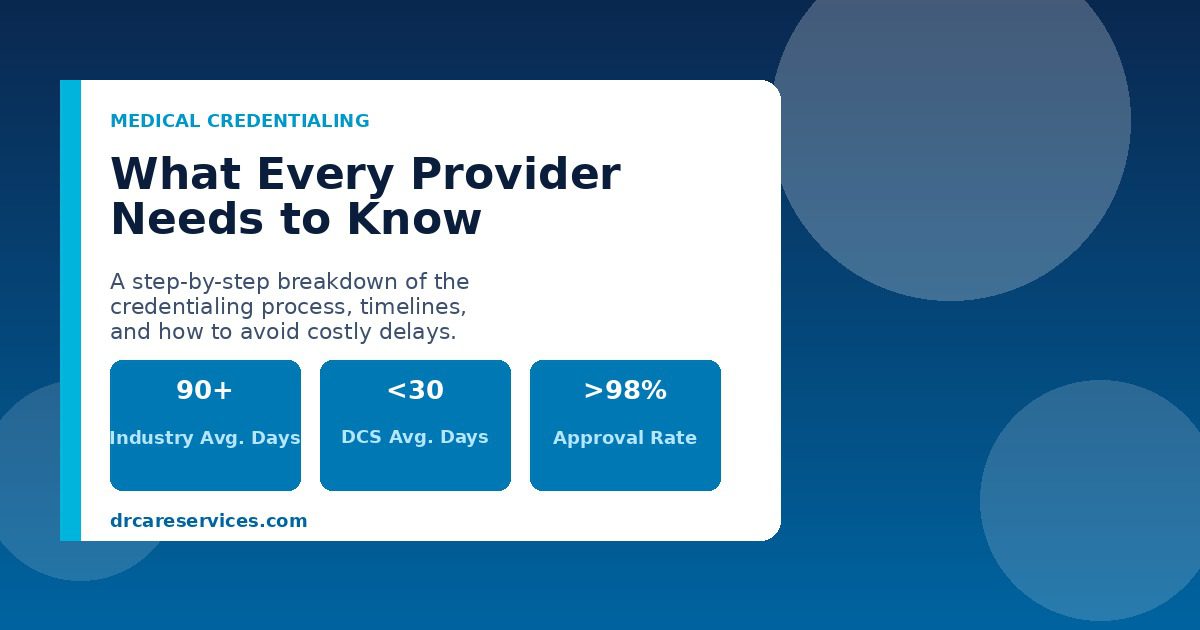
90–120
<30
>98%
Revenue Protection
Every day a provider sees patients without active payer credentialing is a day your practice cannot bill for those services. In most cases, insurance companies will not retroactively reimburse claims submitted before credentialing is finalized. That revenue is simply gone.
Patient Safety and Trust
Credentialing is designed to protect patients from providers who lack the qualifications they claim to have. Rigorous credentialing has been shown to reduce patient safety incidents significantly, and it is the foundation of patient and institutional trust in any healthcare setting.
Legal and Regulatory Compliance
Operating with uncredentialed providers exposes your practice to serious liability. Negligent credentialing lawsuits can result in substantial damages. Regulatory bodies like CMS can impose penalties, and accreditation bodies can revoke hospital certifications if credentialing standards are not met.
Payer Network Access
Being in-network with major insurance payers dramatically expands your patient base. Patients actively seek in-network providers to minimize out-of-pocket costs. Credentialing is the only path to that in-network status — and the patient volume that comes with it.
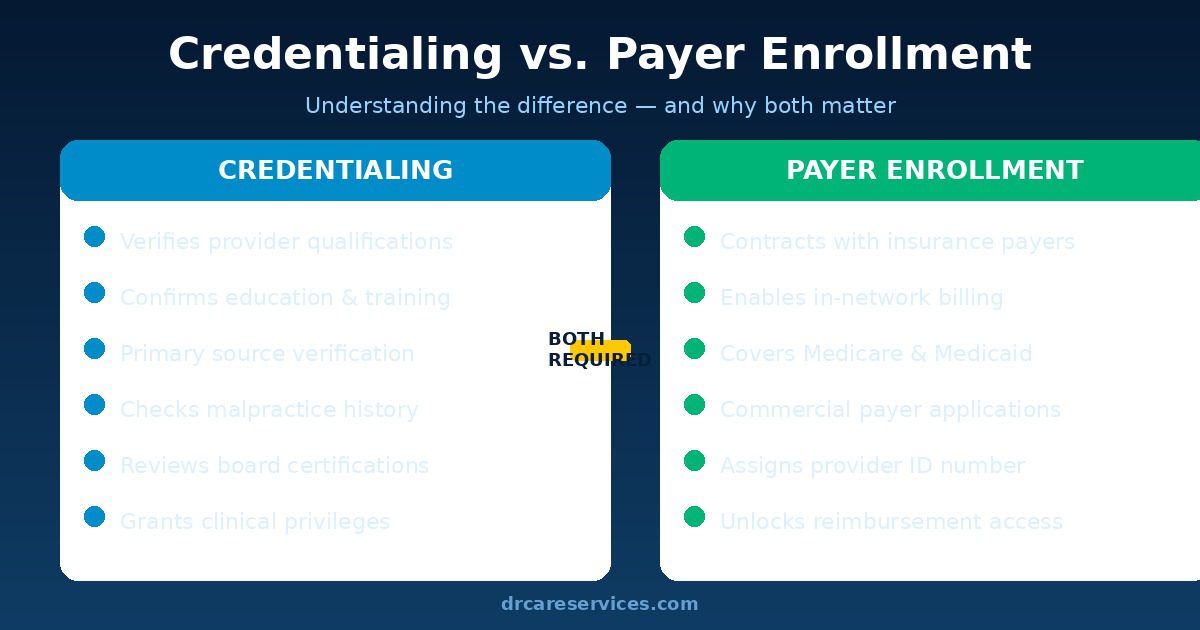
Types of Provider Credentialing Explained
Most articles treat credentialing as a single process — but in practice, there are two distinct types, each with its own requirements, timelines, and governing bodies. Understanding the difference prevents confusion and prevents costly mix-ups.
1. Hospital Credentialing (Clinical Privileges)
Hospital credentialing is conducted by healthcare facilities — hospitals, surgical centers, and large health systems — to verify that providers have the qualifications to perform specific procedures and services within that facility. This is the process that results in the granting of “clinical privileges.”
Privileges are specific — a surgeon might be credentialed to perform a laparoscopic cholecystectomy but not a cardiac procedure. The hospital’s medical staff office manages this process, typically governed by the medical staff bylaws and subject to Joint Commission accreditation standards.
2. Payer Credentialing (Insurance Enrollment)
Payer credentialing is the process insurance companies use to verify a provider’s qualifications before enrolling them in their network. This is what allows a provider to bill Medicare, Medicaid, and commercial insurers like Aetna, Blue Cross Blue Shield, Cigna, and United Healthcare.
Each payer has its own application process, timeline, and requirements. A provider joining a new practice must complete payer credentialing with every insurer whose patients they plan to see — there is no universal shortcut, although CAQH ProView (discussed below) significantly streamlines the commercial payer process.
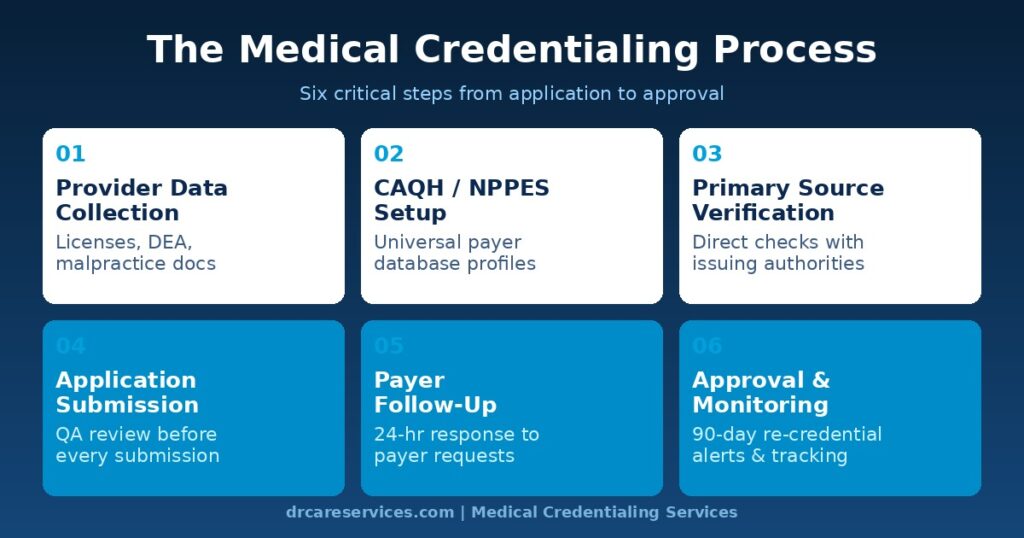
The Medical Credentialing Process: Step by Step
While specific requirements vary by organization and payer, the core credentialing process follows a consistent sequence of six steps. Delays at any stage cascade forward and extend your overall timeline.
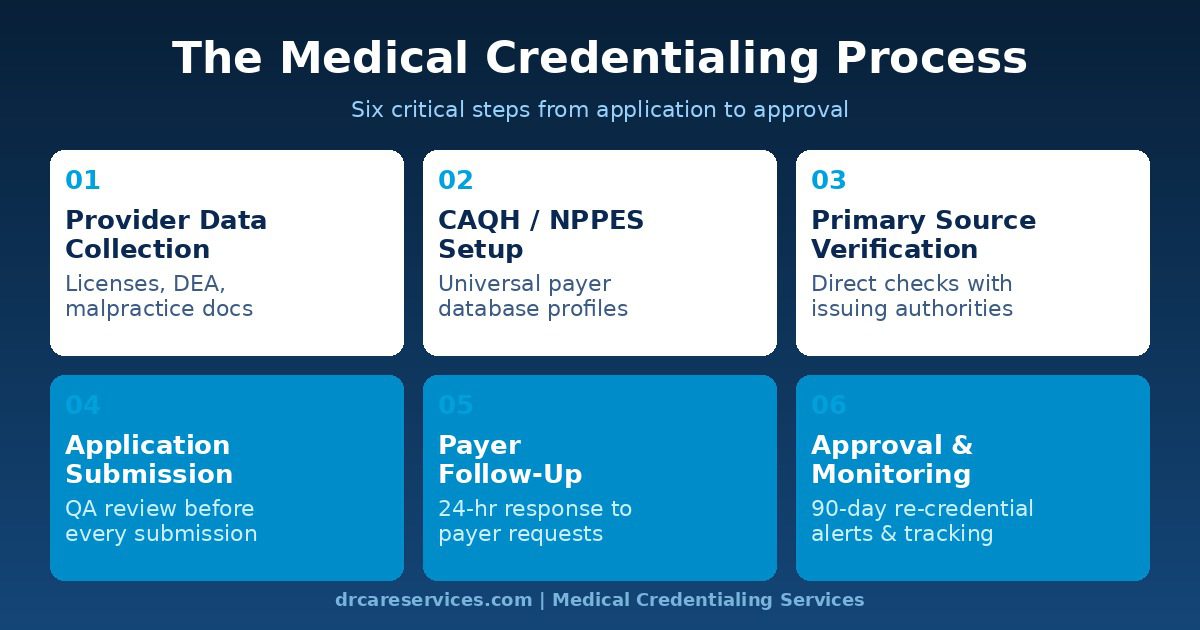
Provider Data Collection
The credentialing process begins with gathering all documentation related to the provider’s professional background. This includes medical school diplomas, residency and fellowship certificates, state medical licenses, DEA certificates, board certifications, malpractice insurance policies, and a comprehensive work history. Accuracy at this stage is critical — any error or omission in the initial data collection will cause delays downstream.
CAQH, NPPES, and PECOS Profile Setup
For most commercial payers, credentialing begins with the provider’s CAQH ProView profile — a universal database that more than 1,000 health plans use to streamline credentialing. For Medicare participation, providers must be registered in NPPES (for their National Provider Identifier) and enrolled in PECOS (Provider Enrollment, Chain, and Ownership System). These profiles must be complete, accurate, and regularly attested before applications are submitted. Outdated or incomplete profiles are one of the single largest causes of credentialing rejections.
Primary Source Verification (PSV)
Primary source verification is the cornerstone of the credentialing process. Rather than accepting copies of documents at face value, credentialing organizations contact the original issuing institutions directly — medical schools, state licensing boards, residency programs, certification bodies, and malpractice carriers — to confirm that every credential is authentic, current, and unencumbered. This protects against fraudulent or exaggerated credentials and is required by NCQA standards and the Joint Commission.
Application Submission
Once all credentials have been gathered and verified, applications are prepared and submitted to the target payers — Medicare, Medicaid, and each commercial insurer the provider will bill. Each payer has its own application format, and any error or missing document triggers a rejection. This is why a rigorous quality assurance review before submission is so important. When applications are submitted correctly the first time, approval rates exceed 98%. When they are submitted with errors, the cycle resets — often adding weeks or months to the timeline.
Payer Follow-Up and Status Monitoring
Submitted applications do not manage themselves. Payers routinely request additional documentation, and some simply stall without proactive follow-up from the applicant. Dedicated credentialing specialists check application status with each payer regularly, respond to documentation requests within 24 hours, and escalate stalled applications before they miss critical deadlines. This proactive follow-up is the single biggest differentiator between practices that complete credentialing in 30 days and those that take four months.
Approval, Confirmation, and Ongoing Monitoring
Once approved, the provider receives a confirmation letter or email from the payer, along with a provider ID number needed for billing. But the process does not end there. Every credential — licenses, DEA certificates, malpractice coverage, and payer contracts — has an expiration date. Proactive monitoring and re-credentialing initiation well ahead of each expiration ensures the provider remains continuously enrolled and billing without interruption.
Documents Required for Medical Credentialing
Incomplete documentation is the most preventable cause of credentialing delays. Having every required document organized, current, and digitally accessible before you begin can shave weeks off your timeline. Below is a comprehensive checklist of what most payers and hospitals will require.
Personal and Professional Identification
- Government-issued photo ID
- Social Security Number (SSN)
- National Provider Identifier (NPI) — Type 1 for individuals
- Curriculum Vitae (CV) covering the past 10 years
Education and Training
- Medical school diploma (copy and primary source verification contact)
- Residency completion certificates with program contact information
- Fellowship certificates (if applicable)
- Board certification(s) — numbers, dates, and expiration dates
Licensure and Certifications
- Current state medical license(s) — number, issue date, expiration date
- DEA certificate — number, state(s), expiration date
- CAQH ID and attestation date
- Medicare PECOS enrollment confirmation
Malpractice and Professional History
- Current malpractice insurance certificate (carrier, policy number, coverage dates and limits)
- Five-year malpractice history (list of any claims, even if resolved)
- Work history for the past 10 years, including any gaps with explanations
- Hospital affiliations and privileges history
Background and References
- Professional references (typically three to five from current or recent colleagues)
- Disclosure of any disciplinary actions, license restrictions, or sanctions
- OIG exclusion list clearance
CAQH, PECOS, and NPPES: What You Need to Know
Three database systems form the backbone of modern provider credentialing. Understanding each one — and keeping them current — is non-negotiable for any practice that bills insurance.
CAQH ProView
CAQH ProView is the Council for Affordable Quality Healthcare’s universal provider data repository. More than 1,000 health plans, including most major commercial payers, use CAQH to access provider credentials rather than requiring each provider to submit a separate paper application for every payer.
A complete, up-to-date CAQH profile dramatically accelerates commercial payer credentialing. However, CAQH profiles must be re-attested every 120 days, and any outdated or missing information can cause applications to be rejected. Many practices have experienced significant billing interruptions simply because their CAQH attestation lapsed without anyone noticing.
NPPES — National Provider Identifier Registry
The National Plan and Provider Enumeration System (NPPES) is the federal registry for National Provider Identifiers (NPIs). Every provider who bills insurance must have an NPI — a unique 10-digit number that identifies them across all payers and transactions. Individual providers hold a Type 1 NPI; practices and group entities hold a Type 2 NPI.
NPI registration must be completed before any payer enrollment can begin. Errors or outdated information in NPPES records can cause claim rejections even after credentialing is complete, so the record must be kept current whenever a provider changes their address, specialty, or organizational affiliation.
PECOS — Provider Enrollment, Chain, and Ownership System
PECOS is the CMS system used to manage Medicare provider enrollment. Before a provider can bill Medicare for any service, they must be actively enrolled and approved in PECOS. The process involves submitting form CMS-855 (or its electronic equivalent), verifying the provider’s identity and credentials, and receiving an approval letter from CMS — a process that can take 40 to 60 days on average.
Medicare revalidation — periodic re-enrollment required every five years (or sooner if triggered by a change in enrollment information) — is also managed through PECOS. Missing a revalidation deadline can result in immediate billing suspension, a disruption that is entirely preventable with proper tracking.
How Long Does Medical Credentialing Take?
The honest answer is: longer than most practices expect, and longer than it needs to be when the process is not managed properly. Here is a realistic breakdown by payer type.
| Payer Type | Typical Industry Timeline | With Expert Management |
|---|---|---|
| Medicare (PECOS) | 40–60 days | 15–30 days |
| Medicaid (State) | 45–90 days | 20–40 days |
| Commercial Payers (BCBS, Aetna, etc.) | 60–120 days | Under 30 days |
| Specialty Payers / Regional Plans | 90–150 days | 30–60 days |
| Hospital Privileges | 60–90 days | 30–45 days |
The gap between the industry average and expert-managed timelines comes down to three factors: complete and accurate applications submitted from day one, proactive payer follow-up that prevents applications from stalling, and prior relationships with payer credentialing departments that allow for faster escalation when needed.
During the credentialing window, many practices use a locum tenens arrangement or allow the new provider to see patients under a supervising physician’s credentials as a temporary measure — though this varies by state and payer, and carries its own compliance requirements.
Re-Credentialing: Staying Continuously Enrolled
Initial credentialing gets a provider enrolled. Re-credentialing keeps them that way. Most payers require re-credentialing every two to three years, and failing to initiate the process on time can result in a billing suspension that is just as damaging as never having been credentialed in the first place.
What Triggers Re-Credentialing?
- Payer re-credentialing cycle (typically every 2–3 years)
- State medical license renewal
- DEA certificate expiration
- Malpractice insurance policy renewal or carrier change
- Board certification renewal
- Change in practice address, specialty, or group affiliation
- Medicare PECOS revalidation (every 5 years)
The Re-Credentialing Timeline Problem
Most practices manage re-credentialing reactively — they respond to payer notices rather than proactively tracking expiration dates. The problem is that payer notices are not always reliably sent, and by the time a practice realizes a credential has lapsed, the billing suspension may already be in effect.
The safest approach is to initiate re-credentialing 90 days before any expiration. This builds in enough buffer for the verification and payer review process without risking a lapse. DCS’s ongoing credential management service tracks every expiration date for every provider and initiates re-credentialing automatically at the 90-day mark.
Common Credentialing Challenges and How to Avoid Them
Even experienced practice managers encounter credentialing delays. Most stem from predictable, avoidable mistakes. Here are the most common pitfalls and what to do about each.
Incomplete or Inaccurate Applications
This is the leading cause of credentialing delays. A single missing document, an incorrect license number, or an undisclosed malpractice claim can result in the entire application being rejected and the clock resetting. The fix is a thorough quality assurance review before any submission — ideally by a credentialing specialist who knows each payer’s exact requirements.
Outdated CAQH Profiles
Many providers set up their CAQH profile once and forget about it. When payers pull the profile months later and find outdated information or an expired attestation, the application stalls. CAQH profiles need to be attested every 120 days and updated immediately whenever any provider information changes.
Slow Primary Source Verification
PSV requires contacting medical schools, licensing boards, and other institutions directly. Some are slow to respond, and delays on their end cascade into delays for your application. Experienced credentialing teams know which institutions tend to be slow and build in extra lead time — or use established verification services that have existing relationships with common PSV sources.
Managing Multiple Payers Simultaneously
A provider joining a new practice typically needs to credential with ten or more payers at once, each with different applications, requirements, and timelines. Without a centralized tracking system, applications fall through the cracks. Practices that manage this without dedicated software or credentialing support consistently take longer and make more errors.
No Proactive Re-Credentialing System
Practices that manage re-credentialing reactively — waiting for payer notices or provider prompts — regularly experience lapses that cause billing suspensions. A calendar-based or software-driven tracking system with 90-day advance alerts for every expiration eliminates this risk almost entirely.
Should You Outsource Medical Credentialing?
For most practices — particularly those with more than one or two providers, those in growth mode, or those without a dedicated credentialing specialist on staff — outsourcing credentialing to an experienced medical billing and credentialing partner is not just cost-effective. It is the fastest, most reliable way to protect revenue.
The In-House Credentialing Reality
Managing credentialing in-house requires a staff member who understands payer-specific requirements, CAQH, PECOS, NPPES, PSV processes, and re-credentialing timelines for every provider — while also keeping up with the rest of their administrative responsibilities. Industry data suggests that in-house credentialing consumes 15 to 25 staff hours per provider. Even one mistake in that process can delay billing by months.
What a Professional Credentialing Service Provides
- Dedicated credentialing specialists — not generalist admin staff
- Multi-step QA review before every application submission
- Established relationships with payer credentialing departments
- Centralized tracking across all providers, payers, and expiration dates
- Proactive 90-day re-credentialing alerts and management
- 24-hour response to payer documentation requests
- CAQH, PECOS, and NPPES ongoing maintenance
Before and After: The Impact of Expert Credentialing
| Metric | Before | After Expert Management |
|---|---|---|
| Average credentialing turnaround | 90–120 days | Under 30 days |
| First-submission approval rate | 60–70% | >98% |
| Revenue lost during credentialing gap | $5,000–$20,000/month | Near zero |
| Re-credentialing managed proactively | Reactive / Often missed | 90-day advance notice |
| Admin hours per provider | 15–25 hours | Under 2 hours |
| CAQH profile accuracy | Outdated / Incomplete | 100% current & attested |
Dr Care Services manages all aspects of credentialing — from initial CAQH setup and primary source verification through payer submission, follow-up, and ongoing re-credentialing — for practices across all 50 states. Our credentialing specialists complete the process in under 30 days for most payers, with a >98% first-submission approval rate.
If slow credentialing is costing your practice revenue, explore our medical credentialing services and see how fast your providers can be billing. And if you want to understand how credentialing fits into your broader revenue strategy, our revenue cycle management services provide end-to-end support from onboarding to cash flow optimization.
Stop Losing Revenue to Credentialing Delays
Our credentialing specialists will review your current enrollment status, identify gaps, and get your providers billing fast. Free consultation, no commitment.